During a 6 month period, Egyptian photographer Morsi visited AIDS wards in seven Cambodian hospitals where he met Cambodians, mostly women, who had contracted the virus. He ended up spending months with patients focusing on the human side of their tragedy. Women covered in these story are all dead now, but others have taken their place.
Over half of the world’s 40 million HIV-infected victims are in their adult productive prime of their life. Every year more than 11,000 more people get infected with HIV. While the eastern European countries and Asia are experiencing an alarming increase in the numbers of victims, Africa south of the Sahara has 25 million known cases which is so far the hardest hit area around the world. In Ukraine the number of people diagnosed with HIV has more than doubled since 2000 and today the country has the hardest hit in Europe. In Cambodia also it is estimated that around 1% of the population have HIV- AIDS, although the real numbers might be much higher. The women in Cambodia are facing one of the hardest cultural challenges in Asia; the cultural code “Chbap Srey”* from the mid 19th century, placing them at a lower position than men. This code also contributes to the fact, that Cambodia has the highest rates of domestic violence with thousand of women are being raped, tortured and physically abused by their husband or close male relatives. Women are not bound by law to obey the cultural code, but it also does not protect them from the invasive punishment they encounter from there society.
Srey Pleng
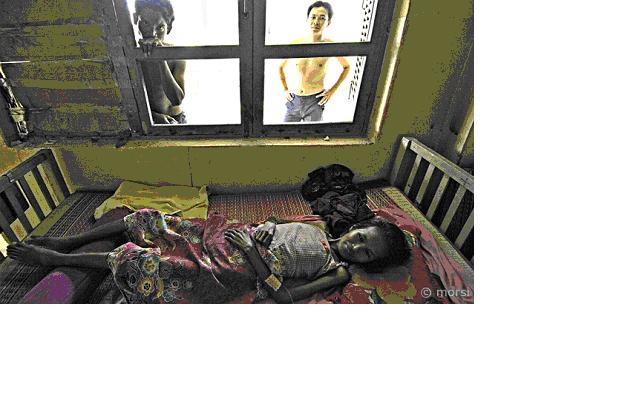
The Srey Sophorn hospital was filled with noise and the smell of disinfectants. Next to an old Toyota Land cruiser, belonging to the French MSF, people were eating lunch with the smell of burnt corpses from the nearby Buddhist crematorium. At the back of the complex I found hospital’s AIDS ward. The patientswith HIV- AIDS seemed pale and exhausted. Every movement required extreme effort and most of the patients just hung out. Most looked like they didn’t notice the world around them, however, every time I entered the room I was met with a stream of careful smiles. They moved Srey Pleng to another room, due to the lack of space. She didn’t like it. It was the male ward. Srey Pleng was 49 years old and was tested positive a year ago she got the infection from her husband few years before He died. Her youngest daughter Luot Sal Lge comes every day to take care of her mother and doesn’t attend any school. When I saw Srey for the first time, she had just been carried into the room, wrapped in her hammock. She looked like a human, whose soul had already found a channel out of her physical body. She had open wounds in her nose and mouth and flies were relentlessly trying to sit on the wounds.
Luot sat behind her mom and watched me. She then tapped her mom on the shoulder and whispered something in her ear. Srey opened her eyes and stared straight into me. Then she smiled with great effort. With this the end of her lips cracked and blood accumulated into a large drop which slowly crept down her cheek. I asked her if she was angry at her husband. My interpreter translated her tears: ‘No, she has forgiven him’.
Rom Chantol
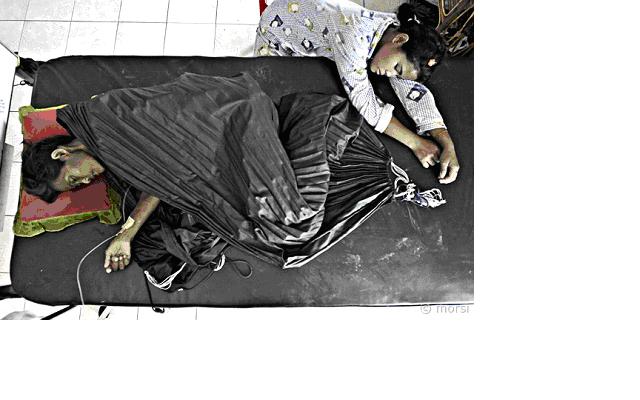
Rom Chantol was 29 years old at the worn out ‘Russian hospital’ in Phnom Penh. The crowded hallways make this place look like city hall. If relatives didn’t come to look after their loved ones, the system would collapse and patients would not receive the care they need.
Rom was strongly affected by the diseases. She looked like a malnourished child in the wide wooden IKEA bed but she smiled at me all the time and made my time with her a pleasure.
Like the rest of the women I met, Rom came from a small village. In her case the Preveng district, not far from Phnom Penh. Her husband, unlike her, didn’t have full blown AIDS, but he has had HIV for the last 4 years. Rom was a housewife and didn’t know she had AIDS until the last stage. Her family took her to a clinic where a blood sample confirmed the doctors’ initial diagnosis. Her husband admitted having unprotected sex with a prostitute and a week later his test also came out positive. Working in the the salt mines in Kampot; South Cambodia her husband was aware about AIDS before the fatal visit to a prostitute, but he was drunk in a small town with no contraceptives at hand and hadn’t seen his wife for six weeks
“But what do I know about time and money?
Rom Chantol dreams her disease would disappear.
“I dream about my little garden before I go to bed – every day”, she said. “I have onions, cabbage and watermelons but I guess the kids in the village have probably eaten the whole lot by now” and then she laughed gently.
She was very angry with her husband in the beginning.
“Buddha shows me the way and that’s how women are raised in Cambodia. I have to forgive my husband. That’s just the way it is”. I asked her what she wanted to tell other women about AIDS, she replied. “Some women are better at taking care of their husband than I was. They must also remember to look after themselves”.
Rom Chantol had only fallen in love with one man in her entire life and married him. This man became the reason for her end. He came and slept on the floor next to her every day and when I asked him what he thought would happen he replied. “I come here to see what will happen to me”
Chan Sokny
The last patient I want to talk about is Chan Sokny. He is 34 years old and caught the disease from his first wife, who died ‘mysteriously’. Then he married his next wife and transmitted the virus to her. After he had been diagnosed HIV positive, Chan visited more than 20 girls over a period of six months.
He always had unprotected sex and if the girl refused he would find someone else. Usually a double payment (less than three American dollars) would turn on any girl.
Chan Sokny was at Calmette, the largest hospital in Cambodia and the central hospital in Phnom Penh. Even with the usual crowds it was a fair place, not as worn out and dirty as the Russian hospitals. The room was filled with families cooking for their relatives. People sat on the beds and the floor and leftover scraps and buckets of spits littered underneath the beds. Chan Sokny wanted me to tell his story so they didn’t make the same mistake. Regarding the multiple visits with the prostitutes he replied. “I was angry with my wife. My first wife. I was angry at women. My interpreter and now close friend added that anger was a very bad thing in Buddhism. “Every day I dream the same dream. I am swimming with my friends in the river. We did that every day. I still do it” he said. In the time I sat with him that day he never spoke a single word to his wife. She looked at him, but he never looked in her in the eyes. Not once.
Are we really that different as individuals or do we act on predetermined patterns of society and what they allow us? Why could these men not protect themselves and their wives? How could the women forgive them? Are our dreams and thoughts similar when we are faced with death? Why do we dream about our childhood and why do dreams turn simple when faced with the inevitable and probably the opposite when our daily lives turn trivial? This are some of the questions I ask myself when I think back about those people.
This article has been perceived and photographed by Morsi, an Egyptian photographer and written Tiarna-lee Hughes, a freelance Writer
*Chbap srey stipulates that an ideal woman (srey krab lakkana) is shy and reserved,does not go out alone and moves quietly without making a noise with her silk skirt, but can identify the merits of her husband and provide him with tactful advice. Chbap srey also stipulates ideal female sexuality: that is women should remain chaste until marriage, and, once married, should be faithful to their husbands. Mohammad Khairul Alam
The HIV/AIDS epidemic has developed into a major warning to human development— mainly in the poorest countries of the world. It spreads out depend on several social custom or norm prejudicial practice, such as gender discrimination, sexual violence, early marriage, trafficking, unsafe sex or exploitation of sex workers, transmission of other STDs, intravenous/injection drug uses. Socio-economic position and illiteracy also can makes vulnerable for HIV/AIDS. It is not only a public health issue but also one which is beginning to affect the dynamics of social, cultural, economic and developmental pace of the society we live in.
In the early days of the epidemic, men vastly outnumbered women among people infected with HIV. In 1997, women made up 41% of all people living with HIV. Today, nearly 50 percent of the global population of HIV infected persons are women. AIDS is now a leading cause of death among women aged 20-40 in Europe and North America. Worldwide, half of all new HIV infections are in young people aged 10 to 25, with teenager girls in some places as much as five times more at risk than teenager boys. The epidemic’s ‘feminization’ is most apparent in sub-Saharan Africa, where close to 60% of those infected are women, and 75% of young people infected are girls aged 15-24.
Being a girl or a boy, a woman or man, influences the nature of the risk for contracting HIV/AIDS and how a person experiences it. First, women are more physically susceptible to HIV/AIDS infection than men – male-to-female transmission during sex is about twice as likely to occur as female-to-male transmission. However, relatively simple precautions can be taken to reduce the likelihood of HIV transmission during sexual activity, so this physiologic disadvantage is not a sufficient explanation for the rising inconsistency in the way men and women are infected and affected by HIV/AIDS.
African women are 2.5 times more likely to become HIV-infected than their male counterparts. This vulnerability to the disease is heightened by the high-risk behavior of the men; due primarily to inadequate knowledge about HIV/AIDS, poor resource-base and insufficient access to HIV prevention services, inability to negotiate safer sex and a lack of female-controlled HIV prevention methods including microbicides. Among the women, this situation is most noticeable among women during their childbearing ages of 15-Up.
There are larger numbers of commercial female sex workers (CSWs) is operating all over the country, Bangladesh, significantly increases the risk of bridging the high risk groups and moving infection into the general population. Men, who frequently visit commercial sex areas and have sex with female sex workers and also with their wives, function as a bridging population and significantly aid the confluence of HIV/STDs into the general population. While, the majority of AIDS cases In Bangladesh are the results of needle sharing.
Commercial sex is often considered as the highest risk segment of the population whereby one could get HIV or STD due to the high-risk sex activity itself and the often-additional injurious high-risk behaviors practiced by sex workers e.g. IDU. CSWs are the principal transmitters of HIV in many countries.
In some countries, including Bangladesh, presence of prostitution and sexually transmitted infections (STIs) is systematically denied, being considered a taboo by the majority of the society. There is no official record of the prevalence of residence base & fleeting sex workers in Bangladesh. Lack of any reliable records of the underground sex industry makes the data shaky. Sex workers in Bangladesh are suffering from unavailability of medical services and knowledge about STIs. Social stigmatization stops these resource-deprived women from seeking proper medical care.
In Bangladesh, commercial female sex workers (CSWs) are among the most vulnerable groups. Most of them CSWs are the age of teen. Their profession exposes them to tremendous risk and increases the likelihood of their partners/customers also being infected. The Rainbow Nari O Shishu Kallyan Foundation and ‘Society for Humanitarian Assistance & Rights Protection’ (SHARP) jointly survey focuses on the attitude, behavior and practice of commercial sex workers in Goalondo Brothel, this study did point out that almost 53% of sex workers enter the profession before the age of 20 years, and 30% enter between 20 to 25 years of age.
Bangladesh is still considered as a low HIV/AIDS prevalent country; but everyone buying sex in Bangladesh is having unprotected sex some of the time, and a large majority don’t use condoms regularly. The fourth national surveillance also found a high prevalence of syphilis among female sex workers. The same floating sex workers in central Bangladesh who had a 0.5 percent prevalence of HIV, for example, had a 42.7 percent prevalence of syphilis. Bangladesh mostly needs comprehensive approach to both sex worker’s rights and deal with HIV/AIDS crises. HIV/AIDS prevention programme, to be truly effective, must include parallel economic and educational initiatives for sex workers. If HIV continues to infect sex workers, it will have an all-round effect on our economic development and also on the overall income of the family. Because, sex workers in Bangladesh gets a high number of client in a week.
References: WHO, UNICEF, CDC
Case studies on HIV-AIDS in Cambodia
Subscribe to:
Post Comments (Atom)
No comments:
Post a Comment